IAS 2023 – Reflections on Day 2
Hello again from Michael and Joe!

G’day and welcome to our summary of the second day of the IAS Science conference from POZabilities and the San Diego HIV Consortium. Today’s blog is led by Joe Caperna, MD.
All sessions started with respect for first nations. ‘I’d like to begin by acknowledging the Traditional Owners of the land on which we meet today, the (people) of the (nation) and pay my respects to Elders past and present. ‘
Today’s highlights included more on Doxy-PEP, bnAbs(1), U=U(2), growing incidence of highly resistant gonorrhea, weight gain with INSTI’s, possible hypertension with INSTI’s and our first protest demanding zero transmissions.
We met new and old colleagues. We saw Dr Andrew Zweig from AHF San Diego and will lunch with him tomorrow. We keep running into Jeff Taylor from PS. I’ve run into quite a few UCSD or UCSD alum researchers, like Lucette Cysique (who led the Neurocognitive talks yesterday) and Dr Richard Haubrich, now at Gilead. WHO Director-General’s keynote speech, The honorable Mark Butler, IAS President Professor Sharon Lewin.
More studies were reported on Doxy-PEP (Doxycycline Post Exposure Prophylaxis), which greatly reduces the risk of Chlamydia and some for Syphilis in MSM. Doxy-PEP treatment is 200mg of doxycycline after sex. Doxycycline is used often for acne and malaria and known to be safe. There was one study, however, that showed failure of Doxy PEP in young women in Kenya. Adherence was good, but the concentrations of doxycycline in the female genital tract were not high enough to prevent STI’s. It is still not known if Doxy-PEP will prevent gonorrhea, but researchers are skeptical. One speaker recommended Doxy-PEP not more than 3 times per week, but did not say why. For now, CDC(3), California Dept of Health(4) and San Francisco Dept of Health(5) recommend that it is still best w/in 24 hours but more than every 24 hours, and must be within 72 hours.

bnABS (Broadly Neutralizing Antibodies) involves the use of specially targeted antibodies to block the virus from infecting the cell. Information was presented on bnABs as PrEP and shown to be partly effective but probably will need combinations of several antibodies to cover the many HIV variants. There were results nearing 100% clearance with 3 bnAbs. Also reported, resistant gonorrhea is increasing.
There were 3 studies on weight gain and ARVs. The first two showed no change in weight or blood pressure related to the ARV. The 3rd study showed that weight gain explained the hypertension. The BMI and hypertension risk is not different for what type ARV regimen. The hypertension is probably weight gain that would have occurred without ARV’s ie, from lifestyle, diet and exercise.
One researcher studied weight after INSTI was switched to a PI. There were 103 patients on DTV/FTC/TAF (dolutegravir, emtricitabine, tenofovir alafenamide) were switched to the PI DRV (darunavir). Results at week 24 showed weight gain may not be reversible with this switch. But who would expect weight loss on a PI? The studies were about what happens if drugs are changed. None showed benefit. Nonetheless, weight needs to be managed.
Hypertension was also looked at related to ARV’s, specifically dolutegravir and TAF.
Researchers found increases in blood pressure and weight with DTV/FTC/TAF, then switched dolutegravir to efavirenz. The study was done in Cameroon with over 600 patients, where they must purchase their own medicines. They could not discern if the hypertension was from the medicines or weight gain that might have happened even if never took the ARV’s. We don’t use efavirenz much if at all anymore in the United States.
An audience member asked about Ozempic and other weight loss drugs. A lot of providers are using these new agents. Researchers studied regimens that had both dolutegravir and TAF and did not know if weight gain was from INSTI or TAF.
The plenary session on HIV Elimination through prevention was very useful. It started with the first protest we saw

We endorse freedom of expression as an essential principle in the HIV response). Most medical doctors in Thailand are unaware of U=U. Their message was “to be confident about U=U.” “There is clear science to support no transmission” at HIV RNA <1000. (Lancet 2023) The protestors were dynamic and got audience to participate, and yell “Zero.” They chanted “On your mark, get sex, we are ready to say zero”. The activists got us excited about getting to zero transmissions. Best part of the conference for us so far. Some of the protesters got up to speak. One said they were infected at birth, another married and planning to have children.
Smallpox is the only infection that we have gotten to zero, but smallpox is very different, no reservoir, short infectious period, versus HIV which has many reservoirs and long infectious period. Also, there is no HIV vaccine.
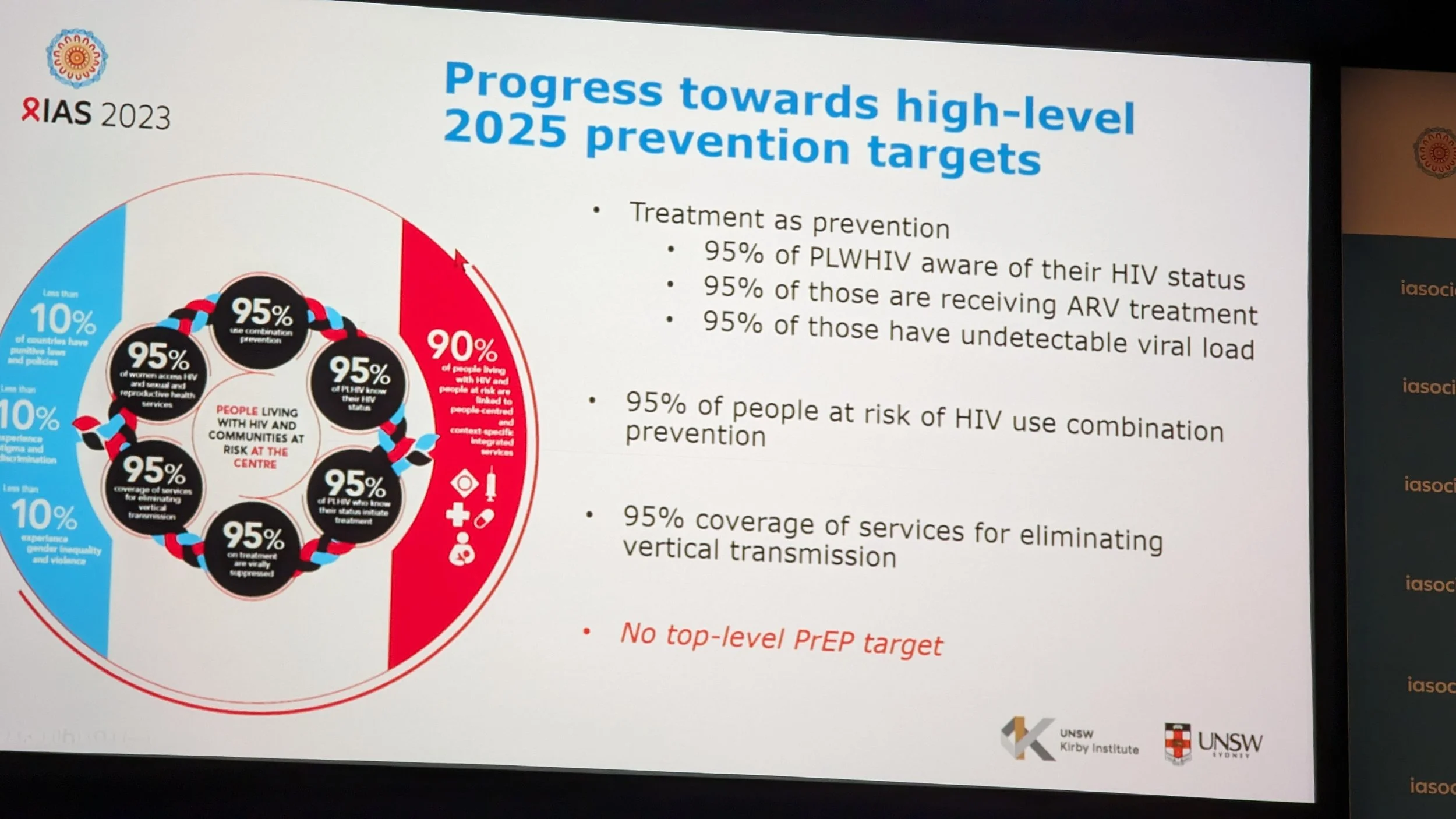
The WHO global target is “ending aids threat by 2030” and decrease the incidence by 90% by 2030, and 95% of at risk populations on combination PrEP.
We want to comment more on yesterday’s presentation of REPRIEVE, which showed a large reduction in heart attacks and strokes with a statin called Pitavastatin. REPRIEVE data on CIS females will happen soon. The investigators noted that women with HIV are under-represented in clinical research trials in general. For context, 53% of individuals living with HIV worldwide are women. We know there are sex-based differences influence HIV infection, HIV care, and the development of HIV-associated complications, like heart disease.
The percentage of women in clinical research trials by trial type was: 19%, in antiretroviral therapy trials and 11.1% in trials of HIV CURE.
Women with HIV have a three-fold risk of having a heart attack compared to women without the virus.
The REPRIEVE trial will test how female-specific hormones influence heart disease risk and the effects of heart disease prevention strategies.
It’s the end of day 2 now, and we learned a little more, and were encouraged by the activists. Prevention, heart disease, hypertension, weight gain, bnAbs, women and activism were highlighted. Honestly, nothing earth-shattering. Tomorrow, we will look for the cure. One encouraging researcher commented “we just don’t know. Tomorrow, we might have our Einstein, who sees HIV in a different way.” Michael said “I might find it hidden under the rug tomorrow.”

You can access the program and schedule online: https://programme.ias2023.org/
Thank you for reading, more tomorrow.
Michael Donovan (Pozabilities) and Dr Joe Caperna (SDHIVC)
Footnotes
1 Broadly neutralizing antibodies (bNAbs) are a type of antibody that can recognize and block the entry of a broad range of different strains of HIV into healthy cells.)
2 U=U People cannot pass HIV through sex when they have undetectable levels of HIV. This prevention method is estimated to be 100% effective as long as the person living with HIV takes their medication as prescribed and gets and stays undetectable. This concept known as Undetectable = Untransmittable (U=U).)
3 CDC Doxy-PEP statement on Doxy-PEP, not GL. https://www.cdc.gov/nchhstp/newsroom/2022/Doxy-PEP-clinical-data-presented-at-2022-AIDS-Conference.html
4 California Dept of Health Doxy-PEP GL’s https://www.cdph.ca.gov/Programs/CID/DCDC/CDPH%20Document%20Library/CDPH-Doxy-PEP-Recommendations-for-Prevention-of-STIs.pdf
5 San Francisco Dept of Health Doxy-PEP GL’s https://www.sfcdcp.org/wp-content/uploads/2022/10/Health-Update-Doxycycline-Post-Exposure-Prophylaxis-Reduces-Incidence-of-Sexually-Transmitted-Infections-SFDPH-FINAL-10.20.2022.pdf