Thoughts on the HIV and Aging Workshop – Washington, DC – Day 1

Over the past 2 days, i attended the HIV and Aging workshop at the ne Johns Hopkins building in Washington, DC (the former Newseum). While there were no major releases of new information, the conference was thoughtfully planned and covered a number of important topics worth passing on. The conference was held in a hybrid format and was one of the more successful hybrid events I’ve attended in a while. Dr Joseph Caperna attended many of the sessions virtually (do you sleep?) and has contributed to this blog. The researchers at UCSD ACRC and HNRP were among the organizers and were well represented in the discussions.
The conference covered a number of key topics; Sarcopenia and Mental Health issues on day one and long acting medications, cardiovascular implications and neurocognitive impacts on day two. There were also poster lightning sessions allowing exciting young researchers from around the world to present summaries of their research projects.
Sarcopenia, Exercise and Accelerated Aging
A general definition of Sarcopenia is ‘age-related loss of muscle mass and strength.’ There is no consensus on the definition, how to diagnose, what tests to use, or how to prevent the condition; however that’s not to say there is nothing that can be done to positively impact the condition.
The session began with an overview of changes in muscle composition in aging, mostly non-specific to HIV. Basically, as we age the types of muscle fibers slowly change from those most suited for speed and strength to fivers whose characteristics include endurance and slower response. There is also an increase in fat infiltration in the muscle fiber, leading to lower muscle mass. The other speakers talked about how to measure and the impact of exercise and nutrition as the most effective approaches to slow and recover from muscle loss. Dr Jung focused on the impact on Mitochondria which are important in that they have a key role in providing power and regeneration/recovery of muscle tissue. As we age or suffer damage to the function of these cells (such as with the old “D” drugs) we see loss of muscle mass and strength.

Exercise is important in building and retaining mitochondrial function and thus muscle mass and strength. It appears that HIIT (High Intensity Interval Training) is most effective in stimulating these cells where normal exercise may have little or no impact. This does not suggest a lack of benefit to lower intensity exercise, it just means it may have limited impact on mitochondrial function. With apologies for the photography challenges, here is a slide I found informative on the impact of diet and exercise on weight related issues.
A lot of the morning discussion was around the early onset of frailty in PLWH and the impacts of both HIV and medication on accelerated loss of muscle mass and strength. It is worth noting that several speakers touched on the fact that while undetectable viral load does mean that the viral particles present in the body may not be able to reproduce and cause a new infection, they are still present and these non-reproducing virus particles may still have an impact on the body with regards to an inflammatory response for example. It was not clear that there is a good understanding of this phenomena.
Mental Health and Cognitive Frailty IN PLWH
The second half of Day One was a session sponsored by the NIH institute on Mental Health and the Division of AIDS. While a lot of this was basic science and not really actionable clinically, there were a few interesting observations that struck me as worth pursuing.
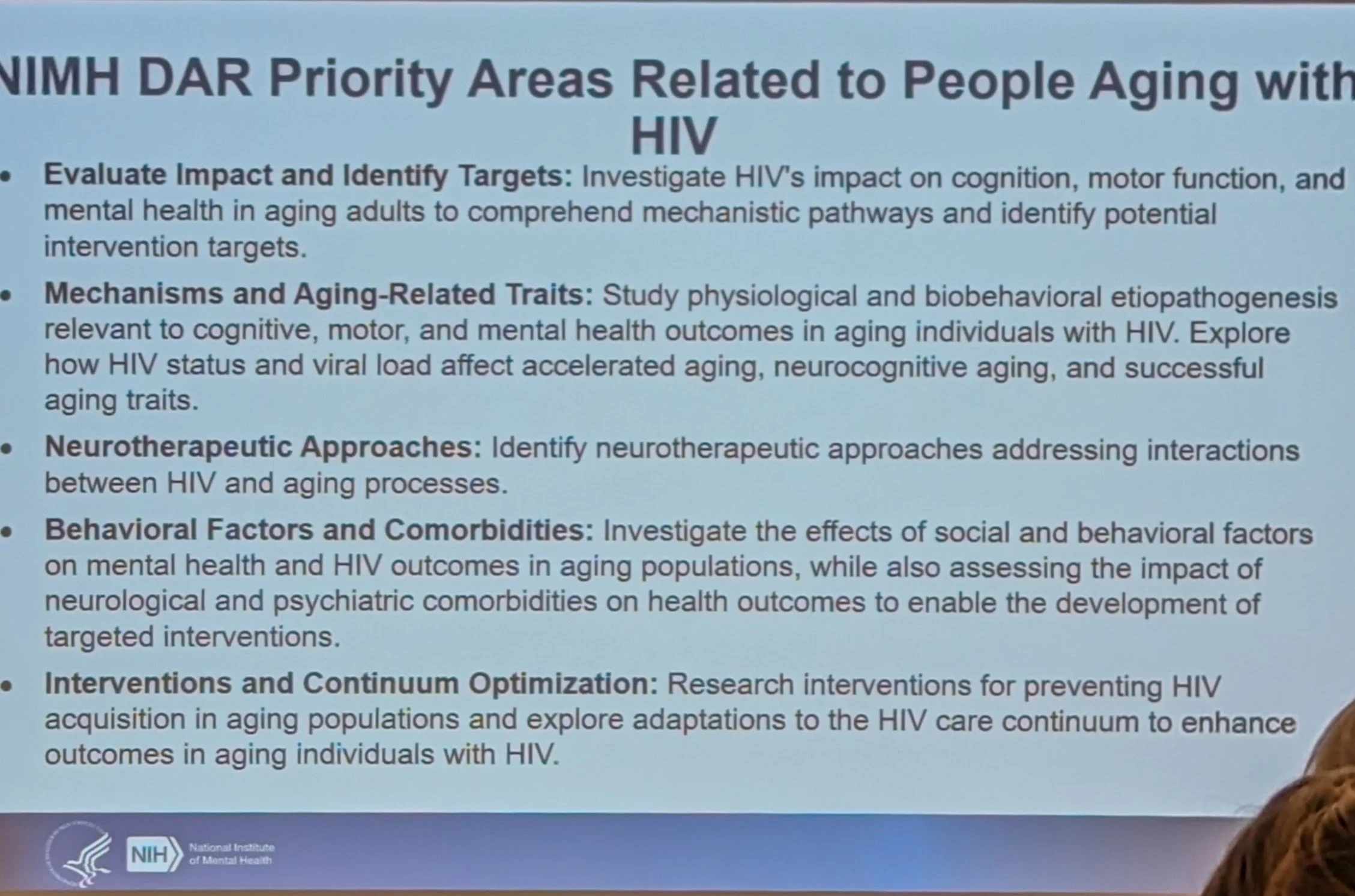
Here is the agenda the NIH provided for their work on HIV and mental health issues:

The impact of depression on accelerated cognitive decline appears to have almost the same impact on mortality among PLWH as does adherence to ART. This points to the criticality of identifying and treating symptoms of depression in PLWH as part of the standard of care.
There was a good deal of discussion around the impact of perceived quality of life, stigma and the impacts of access to quality food, housing and a safe environment on the degree of cognitive frailty. While there was the usual discussion of medication intervention, the impacts of both exercise and diet were significant, both from a medical and perception of quality of life. A lot of really good basic science information presented but little truly actionable beyond what I’ve mentioned. We need to ensure people have access to teh basics of living; food, clothing, shelter and can spend time keeping themselves healthy and as active as they are able. We also need to ensure we identify and treat depression.
Day 1 ended with dinner at one of my old favorite restaurants in DC, Cuba Libre…
